
Case Report | DOI: https://doi.org/10.31579/2690-8794/007
1 Department of Internal Medicine, University of Uyo Teaching Hospital, Uyo, Akwa Ibom State.
2 Department of Histopathology, University of Uyo Teaching Hospital, Uyo, Akwa Ibom State.
*Corresponding Author: Taiwo T Shogade Department of Internal Medicine, University of Uyo Teaching Hospital, Uyo, Akwa Ibom State
Citation: Taiwo T Shogade, Asukwo E Onukak, Akpabio A Akpabio, Effiong A Bassey, Idongesit O Umoh, Olatunde Michael Tanimowo et al, (2020) Pulselessness in an HIV Infected adult Female: A Rare Case of Ergotism, 2(1): Doi: 10.31579/2690-8794/007
Copyright: © 2020 Taiwo T Shogade, This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 20 January 2020 | Accepted: 28 January 2020 | Published: 03 February 2020
Keywords: ergotism, doppler, retroviral disease, pulselessness, thrombosis
Abstract: Ergotism can present with vascular, neurologic and gastrointestinal symptoms including gangrene in severe cases. In HIV, toxicity from interaction with protease inhibitors has been documented. We report case of a female who took cafergot for migraine resulting in absent peripheral pulses. She made a good recovery with steroids and pentoxyfilline
Ergotism is a complication of acute intoxication and/or chronic abuse of ergot derivatives. It expresses itself with symptoms ofperipheral vasospasm [1,2].(numbness, tingling, burning pain, pulselessness, gangrene) as well as neurologic (headache, psychosis) and gastrointestinal symptoms (nausea, vomiting, abdominal cramps)[3].This complication occurs more in patients taking ergot derivatives with certain drugs such as protease inhibitors for different indications[4].
A 37-year-old female was referred to our hospital, after she was managed for hypovolemic shock at the referring centre with intravenous crystalloids and hydrocortisone without improvement. She presented with numbness, pain and coldness of the extremities, nausea, several episodes of vomiting, lethargy and generalized body weakness. Physical examination findings were non-palpable peripheral pulses and unrecordable blood pressure.
Additional history revealed that she recently had a bout of migraine headache for which she ingested a total of 8 tablets of over-the-counter Cafergot (Ergotamine tartrate 1mg + Caffeine 100mg) at a dose of two tablets twice daily over 2 days with resolution of the headache, but development of multiple symptoms suggestive of drug adverse effects two days later.
She was diagnosed with HIV infection eight years prior and her antiretroviral drugs regimen at presentation comprised (Lopinavir 400mg/Ritonavir 100mg and Abacavir 300mg and Lamivudine 150mg) taken twice daily for the preceding 3 years with undetectable viral load. She had a 2-year history of migraine headaches for which she was treated and recovered completely from.
At presentation, other possibilities such as peripheral arterial disease, thrombosis and vasculitis were all considered. Peripheral arterial disease was not likely due to absence of diabetes, hypertension and dyslipidemia. Thrombosis was excluded by a normal clotting profile, electrocardiography (ECG), echocardiography (ECHO) findings and Doppler scan result, while a normal erythrocyte sedimentation rate (ESR) and absence of purpura or fever excluded a vasculitis.
Emergency Full blood count, Erythrocyte sedimentation rate, electrolytes, urea, creatinine, fasting lipid profile, ECG and 2-D-echocardiography done at presentation were all normal. She was initially managed as a case of anaphylactic shock with intramuscular adrenaline, dopamine infusion and 20mg of oral nifedipine (she took without doctor’s instruction), then referred to cardiology unit.
At the cardiology unit a diagnosis of peripheral arterial vasospasm secondary to Cafergot toxicity was made. Though there was no facility to do arteriography, Doppler ultrasound scan of her extremities was done though after commencement of treatment showed generalized low resistance waveform and reduced flow volume involving both upper and lower limb arteries with details shown in table one and figure one.
She was commenced on a stat dose of intravenous methylprednisolone succinate 1mg/kg (80mg) in 500mls of normal saline, oral vasoprin 75mg daily, diclofenac 75mg twice a day, and pentoxyphiline 400mg twice daily. Patient started experiencing resolution of symptoms and her blood pressure as well as pulse rate became recordable two days after commencement of these medications (blood pressure 110/70mmHg, pulse rate 88beats/min). She was discharged home nine days post admission after counselling against usage of ergot derivatives. Her last follow-up visit, three months post-discharge, was unremarkable.
Vasospasm is a rare but well recognized complication of ergot alkaloid agents. The term “St. Anthony’s fire” was used in the middle ages to connote ergotamine intoxication following consumption of grain infected with the fungus Claviceps purpurea, which manifested with burning pain and limb necrosis. Ergotism mostly affects the lower extremities, but involvement of the carotid, coronary, mesenteric, and renal arteries has also been reported [5].
Toxicity may occur with ergotamine overdose or with normal doses administered along with drugs that inhibit its hepatic metabolism. Protease inhibitors such as lopinavir/ritonavir combination, which was part of the index patient’s antiretroviral treatment regimen, are potent inhibitors of CYP3A4. CYP3A4 is responsible for the metabolism of ergotamine and when inhibited can result in ergot toxicity[6].
Ergot toxicity has been previously reported in a Caucasian3 and Latin American patients[1,7].Reports from sub-Saharan Africa are scarce though one case was reported recently among 265 West African HIV-infected patients undergoing a protease inhibitor drug trial. The patient was inadvertently prescribed ergot derivatives for headache by a doctor who was unaware of the on-going study[8].In our index patient, self-medication resulted in her symptoms which were possibly worsened and prolonged by vasopressor therapies (dopamine, adrenaline) administered at the referring hospital.
Severe ergotism has been described in patients taking ritonavir, even after a single dose of ergotamine[9].Apart from discontinuing the offending medications, other therapies that have been tried in patients presenting with cafergot toxicity include prostacyclin, pentoxyfilline, nitroglycerin, calcium channel blocker and methylprednisolone.[1,3,4,10].
In severe forms refractory to pharmacological treatment, intra-arterial balloon dilatation or surgical sympathectomy can be effective[7].
In conclusion, It is important to maintain a high index of suspicion especially in HIV-infected patients in order to diagnose this rare but potentially reversible condition. Vasopressors are best avoided as they may worsen symptoms and prolong recovery. Treatment of spasm with methylprednisolone and pentoxyphylline appear to be effective for preventing limb necrosis and amputation.
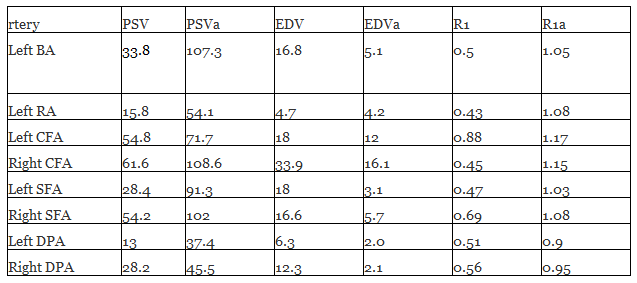
PSV: T-test = -5.978, P-value = < 0>
EDV: T-test = 4.922, P-value = 0.001
R1: T-test = -9.815, P-value = < 0>
BA: Brachial artery, RA: Radial artery, CFA: Common femoral artery, SFA: Superior femoral artery, DPA: Dosalis pedis artery
a: value 10months after, PSV: Peak systolic velocity, EDV: End diastolic velocity, RI: Resistive index.
Doppler ultrasound scan of both upper and lower limb vessels
The upper limb arteries appear normal in caliber, wall thickness, no demonstrable calcification, plaque or focal narrowing from the subclavian arteries to the deep palmar arches and shows pulsatile colour flow in all the arterial segments bilaterally.
Spectral waveform analysis show generalized reduced peak systolic velocity (PSV), low resistance biphasic waveform with loss of early reversal diastolic flow from the subclavian to the Radial and Ulnar arteries bilaterally.
The lower limb arteries also show pulsatile colour flow in all the arterial segments. The arteries appear normal in caliber and wall thickness but show generalized reduced PSV values in all the arterial segments bilateral (left << right PSV=13cm/s>
Spectral tracing shows spectral broadening with low resistant biphasic waveforms and loss of the early reversal diastolic flow in all the arterial segment bilaterally.
The veins of the upper limb appear sonographically normal.
The ratios of the distal-to-proximal PSV is <2>
The upper and lower limb veins show normal colour flow, phasic variation with respiration, compressibility, and flow augmentation and absent reflux flow during valsalva maneuver.
There is no demonstrable supraclavicular, axillary, inguinal or femoral lymphadenopathy. No demonstrable upper or lower limb oedema.
Generalised low resistant biphasic waveforms with reduced flow velocities involving both upper and lower arteries suggestive of vasodilator actions of medication.
Repeat Doppler performed 10months later shows pulsatile colour flow with normal high resistant triphasic waveforms in all the arterial segments of the upper and lower limbs respectively.
Electrocardiography: Normal sinus rhythm
Echocardiography: Normal echocardiography findings
Packed cell volume 40%
Hemoglobin: 15.5g/l
Total white cell count: 9.4X109/L
Platelet: 273X109/L
Neutrophils 69%
lymphocyte 23%
Monocyte 6%
Eosinophils 6%
Creatinine: 66mmol/l
Urea: 3.0mmol/l
Sodium: 143mmol/l
Potassium: 3.2mmol/l
Chloride: 108mmol/l
Bicarbonate: 25mmol/l
Erythrocyte sedimentation rate: 8mm/1st hour
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
